Earlier this month, I spoke at NVIDIA GTC to a room of developers about how NVIDIA’s accelerated computing can help transform the future of healthcare. I opened with a comparison that has stayed with me for years.
In Chicago, life expectancy in the Loop is reported to be about 87 years. In West Garfield Park, it is reported to be about 67.1 These are two neighborhoods, a few miles apart, sharing the same city, and many of the same hospitals. And yet, they have markedly different life expectancy outcomes.
What helps explain this gap?
Part of the answer is operational. When minutes matter, the difference can be whether a system helps teams move from “not sure” to the next step quickly enough. When a patient arrives with a sudden, severe headache, clinicians have to quickly determine whether it’s a dangerous neurologic emergency or a less serious cause.
This is why imaging is so important, because it frequently informs the next step in care.
Stroke makes the point with painful clarity. Here, imaging helps determine whether the stroke is ischemic or hemorrhagic and whether a patient may be a candidate for thrombolysis or thrombectomy, consistent with clinical judgment and applicable protocols. In medicine, we often say, “Time is brain.” Every minute of untreated ischemic stroke is sometimes estimated to cost about 1.9 million neurons.2
If imaging is so central to faster decisions, is the fix simply more scanners?
Unfortunately, not.
More devices can help at the front end, but the bottleneck patients experience is often downstream, at the decision point.
In radiology, the constraint is not the volume of image acquisition. Instead, it’s related to interpretation capacity and workflow throughput. From 2008 to 2019, aggregate radiologist workload in the U.S. was reported to rise by about 80% while the workforce reportedly grew only modestly. 3This means that adding machines can increase volume upstream while deepening the backlog where interpretation, communication, and next-step decisions have to happen.
Take the example of mammography. About 10% of patients are called back, yet only around five cancers are detected per 1,000 screens in commonly cited estimates.4 As follow ups progress, roughly two thirds of biopsies are reported to ultimately prove benign. Each step adds queues, handoffs, and interpretation work. Every step can stretch the time between signal and closure.
At NVIDIA GTC 2026, I presented one practical way to help solve for this problem: a control plane. To understand what a control plane is, think of a cockpit in an airplane. A cockpit does not create lift, and it does not replace the pilot. Instead, it concentrates the signals that matter, standardizes checklists, coordinates automation, and helps keep the aircraft predictable when conditions change.
In imaging terms, the control plane is the layer intended to help keep an AI-enabled workflow predictable. It is designed to keep track of where each exam is, apply the rules that must be met to move forward, coordinate what runs when and where, keeping humans in the loop.
Let’s use the example of autonomous X-Ray imaging to illustrate how teams at GE HealthCare and NVIDIA are working together to help bring a control plane for “autonomous” X-Ray to life.
X-ray is among the most widely used forms of medical imaging, with very large volumes of exams each year. As a result, incremental improvements in consistency and rework can be reflected in customer-felt operational metrics: reduced repeat rates, fewer callbacks for inadequate studies, and shorter time-to-usable images for downstream interpretation.
AI-assisted X-ray5, designed for supervised use, is intended to help extend scarce expertise so more exams reach decision-ready quality on the first pass, subject to appropriate validation, local workflows, and clinician oversight.
An important point: the compute layer is necessary but not sufficient. NVIDIA provides accelerated computing, software to run models at scale, and simulation capabilities. GE HealthCare brings the devices, workflow integration, and processes to support validation and governance for operation across sites. Together, this combination is designed to support day-to-day operational performance measures.
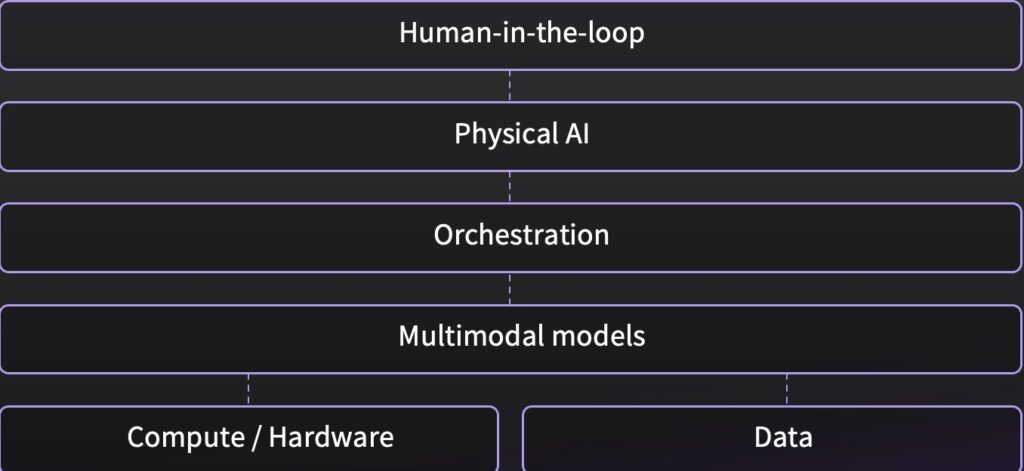
Looking ahead, we are designing the control plane, architecture so that the different layers could work together as outlined below, helping turn the exam into a managed process with defined gates while keeping the technologist in control:
- Predictable edge performance is intended to keep guidance and quality checks immediate during the exam, even when rooms are busy. We run this on edge devices using NVIDIA’s stack: CUDA for fast inference, MONAI for consistent deployment, and Triton for low-latency serving across multi-step pipelines. This could make models run reliably inside real clinical workflows, not as offline one-off tools.
- Workflow guidance is being designed to integrate sensing and on-screen direction into the X-ray room so positioning support is available at the moment it is needed.
- Quality gates are being designed to run before the patient leaves the room by checking required anatomy and flagging motion, rotation, exposure issues, and artifacts early.
- Orchestration and escalation would route each step, record what happened, and escalate to the technologist or clinician when conditions are not met, supporting human oversight while keeping throughput moving.
- Governance at scale could standardize monitoring across sites, tracking repeat rate, callback burden, override and escalation rates, quality failures, and performance drift so improvement can be managed like any other operating metric.
- Release discipline can use MONAI to package the full imaging pipeline as a versioned artifact so updates could be validated, rolled out in stages, monitored, and rolled back when performance shifts.
This is what a control plane is intended to do in practice. It could help increase the capacity of expertise by reducing rework, tightening handoffs, and shortening the path from acquisition to a decision-ready study. And just as important, it can make outcomes measurable and comparable across sites.
This approach can travel beyond healthcare. Most organizations start by asking where to add AI, and they can end up with scattered point tools and fragile integrations. A better starting point is the constraint. Ask yourself these questions: Where does work pile up? What has to remain predictable under surge? Which gates are non-negotiable? Which customer-felt metrics will show the system is helping?
All you have to do to design a great cockpit for your business is start with the constraint, then design the control plane that keeps performance predictable under surge, enforces non-negotiable gates, validates what is deployed, and ties outputs to measurable outcomes.
Bon Voyage.
- Chicago Department of Public Health (CDPH) “Life Expectancy in Chicago, 2023” ↩︎
- Time in Brain: Quantified. https://pubmed.ncbi.nlm.nih.gov/16339467/ ↩︎
- Harvey L. Neiman Health Policy Institute / Journal of the American College of Radiology, 2024) ↩︎
- AJR: https://www.ajronline.org/doi/full/10.2214/AJR.15.15987 ↩︎
- Technology in development that represents ongoing research and development efforts. These technologies are not products and may never become products. Not for sale. Any reported results are preliminary and subject to change. Not cleared or approved by the U.S. FDA or any other global regulator for commercial availability. ↩︎