In women’s health, pelvic MRI is often used to answer high-stakes questions in gynecologic disease, such as whether cervical cancer has spread, whether an ovarian mass has features concerning for malignancy, or whether endometriosis has invaded deep pelvic structures.
The need for high-quality imaging is critical.
Endometriosis – a condition where tissue similar to the uterine lining grows outside the uterus – affects about 10% of reproductive-age women and is often associated with years of diagnostic delay. Cervical cancer remains the fourth most common cancer in women globally, with an estimated 660,000 new cases and 350,000 deaths in 2022. Ovarian cancer presents a different challenge because it is frequently diagnosed after it has spread, when survival is substantially lower than for localized disease.
Challenges in imaging
These conditions share common imaging challenges.
Small lesions can be difficult to detect, deep pelvic structures can be hard to distinguish, bowel motion can blur anatomy, and long or variable exams can reduce image consistency. In endometriosis, these limitations can affect assessment of adhesions, endometriomas, and deep infiltrating disease. In cervical cancer, image quality influences evaluation of the cervical stroma and parametrium, while in ovarian cancer it affects characterization of adnexal masses and other features that may suggest malignancy.
Because MRI can create detailed images of soft tissues without using radiation while showing the body from different angles, high-quality imaging can play an important role in supporting clinical assessment and treatment planning. However, conventional pelvic MRI can be limited by bowel motion, long examinations, variable protocols, and insufficient spatial resolution for small lesions or subtle tissue planes. Because many clinically important assessments rely on detecting very subtle imaging features, the effectiveness of MRI is closely linked to the quality and appropriateness of the imaging protocol used.
For example, radiologists may need to identify a thin preserved rim of cervical stroma when assessing tumor extent. They may also need to detect a small enhancing solid component within an ovarian lesion or determine whether adjacent pelvic organs move independently or appear tethered together, which can indicate adhesions or deep infiltrative disease. These findings can be subtle or hard to recognize if image quality is suboptimal or the examination is not designed properly to answer the specific clinical question.
To support diagnostic assessment, MRI examinations should ideally conform to robust and standardized protocols that are tailored to the disease being investigated. These protocols define how the examination is performed, including the sequences acquired, imaging planes used, volunteer preparation, and the administration of contrast when appropriate. When combined with the inherent strengths of MRI, such protocols can help support detection and characterization of clinically relevant imaging findings.
A protocol-focused research investigation
A research collaboration between GE HealthCare and radiologists at UC San Diego focused on developing optimized female pelvic MRI protocols for three high-impact areas of women’s health: endometriosis, cervical cancer, and ovarian cancer. The protocols were designed to improve visualization of small lesions and deep pelvic anatomy while keeping scan times clinically feasible, with full exams reported at approximately 30 minutes, providing comprehensive imaging within a timeframe that can fit more easily into routine clinical workflows.
At the very outset, we recognized that each disease needs its own protocol. When it comes to endometriosis, accurate detection of deep infiltrating disease depends on optimizing sequences and imaging planes. Cervical cancer requires careful local staging because treatment planning depends on whether tumor extends into adjacent tissues. Ovarian cancer evaluation often depends on distinguishing benign from suspicious adnexal lesions and understanding enhancement behavior over time.
Maximizing image quality
Our MRI protocols are designed to support image quality and help ensure anatomy is clearly visible and reproducible. They include several complementary imaging sequences.
MRI protocols may include several imaging sequences, each providing different information:
High-resolution T2-weighted imaging: Provides detailed anatomical views, helps define the boundaries of organs and lesions, and highlights fluid-rich tissues, making it particularly useful for evaluating pelvic anatomy.
T1-weighted imaging with fat suppression: Suppresses fat signal, allowing abnormalities such as blood products, inflammation, and contrast-enhancing tissue to stand out more clearly while providing complementary tissue detail.
Diffusion-weighted imaging (DWI): Measures the movement of water molecules within tissue and can help identify areas of increased cellularity that may be associated with tumors.
Dynamic contrast-enhanced MRI (DCE-MRI): Acquires a series of images before, during, and after contrast administration to evaluate tissue blood flow and enhancement patterns, assessing how tissue enhances over time.
Because pelvic MRI is especially vulnerable to motion-related artifacts, the protocols emphasize techniques that help maintain image quality and reduce the impact of volunteer and physiologic movement.
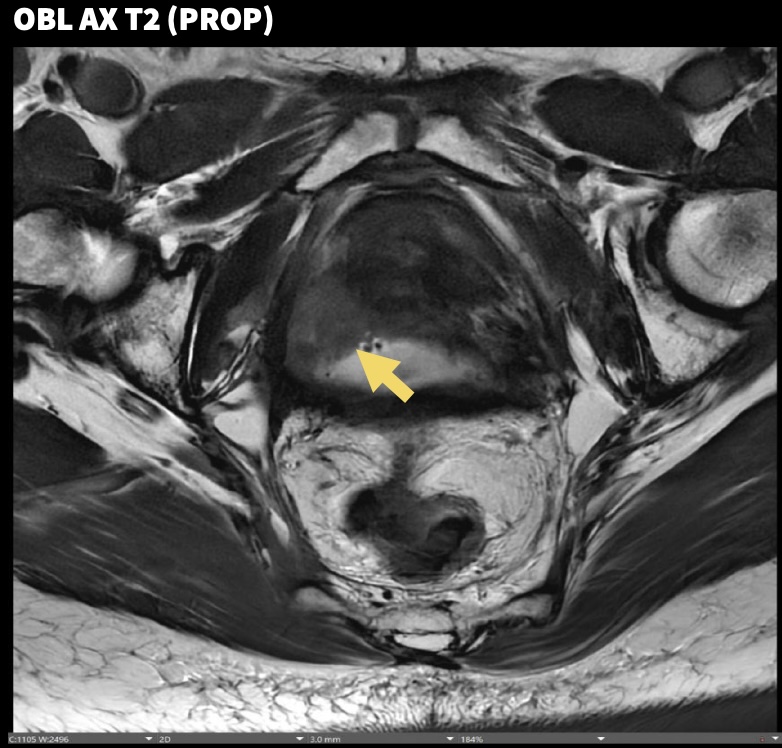
For cervical cancer, the protocol includes oblique axial T2-weighted and diffusion-weighted images oriented perpendicular to the cervical axis. This orientation helps radiologists evaluate the cervical stroma and assess whether tumor extends into the parametrium.
For ovarian cancer evaluation, the protocol emphasizes characterization of adnexal lesions, including dynamic contrast imaging with temporal resolution under 15 seconds. Faster temporal resolution enables assessment of enhancement kinetics, which may assist radiologists in differentiating imaging characteristics associated with benign and higher-risk lesions.
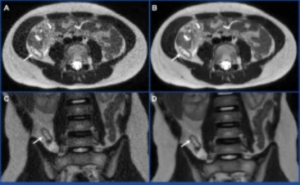
For endometriosis, the protocol adds cine MRI, a dynamic (moving)-image MRI technique used to assess the sliding motion between pelvic organs. Reduced or absent sliding may suggest adhesions, which may be clinically significant in cases of deep infiltrating disease.
Preparing trial volunteers
We also developed protocols to help standardize volunteer preparation, including vaginal gel, micro-enema, and anti-peristaltic agents.
Across the optimized protocols, radiologists qualitatively compared image quality, lesion conspicuity, and diagnostic confidence with prior institutional protocols. In this research evaluation, the optimized protocols were associated with improved visualization of small lesions and delineation of deep pelvic structures.
Our work demonstrates that pelvic MRI can be tailored more precisely to the clinical question without sacrificing practicality. We believe this represents an important step toward a scalable framework for women’s health MRI that recognizes endometriosis, cervical cancer, and ovarian cancer as distinct diagnostic challenges rather than treating the female pelvis as a single generic imaging region.
The statements described above are based on research experience and protocol development activities. Results may vary depending on volunteer characteristics, clinical presentation, imaging system configuration, operator technique, and institutional practice. MRI findings should be interpreted by qualified healthcare professionals in conjunction with other clinical information. The protocols described are intended to support image acquisition and assessment and are not intended to diagnose, treat, cure, or prevent any disease.